The Patient: The details of this patient’s complaints and presentation are lost, but we know he was a 66-year-old man who was being treated in the Emergency Department. His rhythm went from sinus tachycardia with non-respiratory sinus arrhythmia to multi-focal atrial tachycardia (MAT) to wide-complex tachycardia. The WCT lasted a few minutes and spontaneously converted to an irregular sinus rhythm.
Wide-complex tachycardia: Ventricular tachycardia or aberrantly-conducted supraventricular tachycardia? When confronted with a wide-complex tachycardia, it can be very difficult to determine whether the rhythm is ventricular or supraventricular with aberrant conduction, such as bundle branch block. The patient’s history and presentation may offer clues. It is very important, if the patient’s hemodynamic status is at all compromised (they are “symptomatic”), the WCT should be treated as VENTRICULAR TACHYCARDIA until proven otherwise.
There have been many lists made of the ECG features that favor a diagnosis of ventricular tachycardia. Here are two such lists: Life In The Fast Lane, and National Institute of Health.
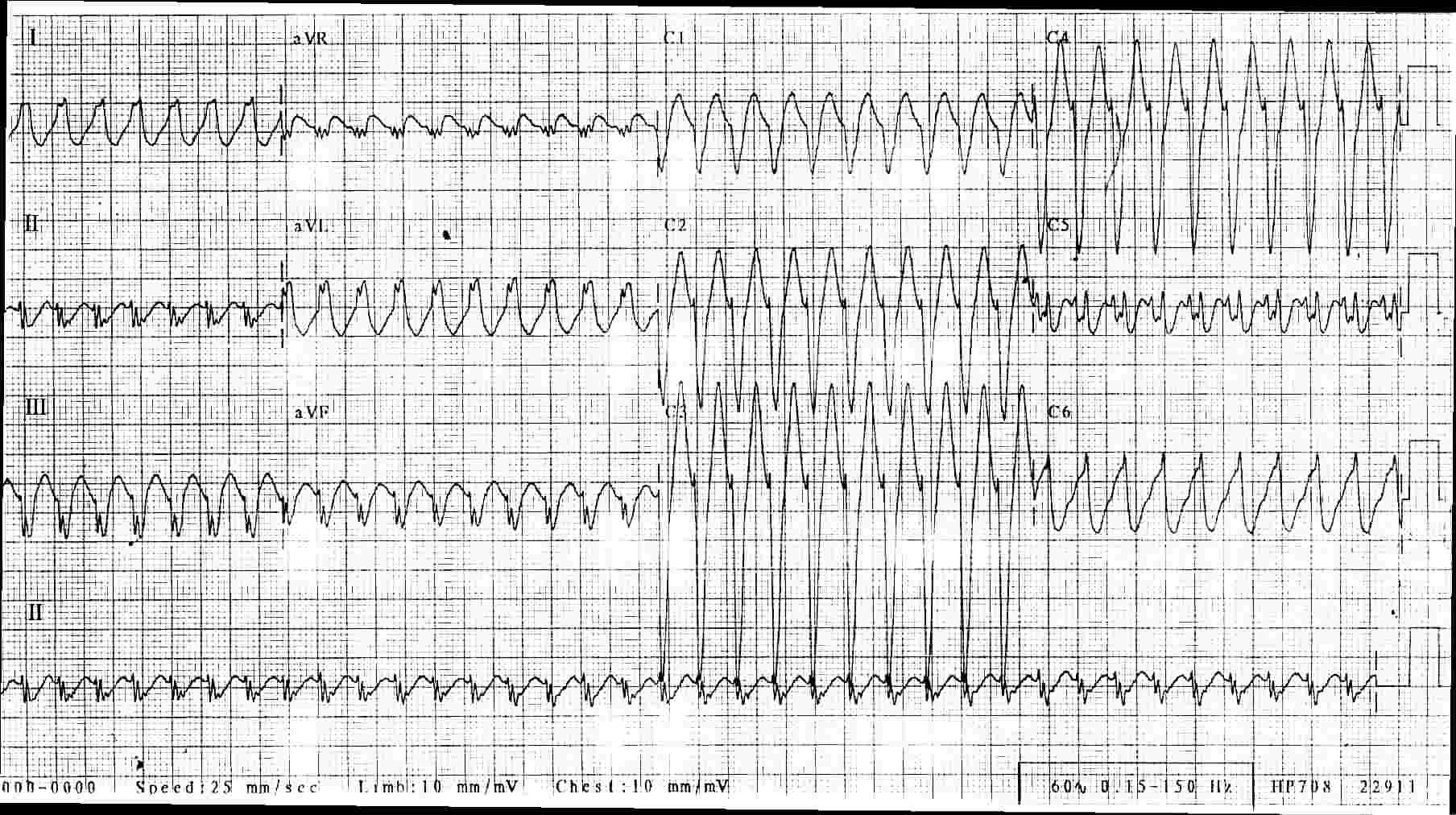
The ECG: This ECG shows a regular, fast, wide-QRS rhythm. The rate is 233 bpm. It had a sudden onset and sudden offset (not shown on this ECG), and the rhythm lasted about 3-5 minutes. The patient felt the change in rate, but did not become hypotensive or unstable. Some features that relate directly to the most commonly-referenced VT vs. SVT charts are:
1) The morphology of the QRS complexes in this ECG is indicative of left bundle branch block. V1 has a wide, negative, monomorphic QRS. Leads I and V6 have wide, positive QRSs. Aberrant conduction often takes a LBBB or RBBB pattern.
2) The QRS is difficult to measure due to unclear start and stop points in all leads, but the overall width appears to be about 120 ms (.12 sec). VT tends to have very wide QRS complexes, greater than 160 ms.
3) This ECG’s axis is about -30 degrees, and aVR is negative. This indicates an axis just a little to the left, within normal range. An extremely abnormal axis, between +180 degrees and -90 degrees (called Northwest axis) almost always indicates VT. Both SVT and VT can have normal axes.
4) The precordial leads V2 through V6 have RS patterns. Any precordial lead havig an RS pattern favors the diagnosis of SVT.
5) The precordial leads transition from negative in V1 to positive in V6, with a somewhat late transition in V5. Precordial concordance (all precordial QRS complexes in the same direction) favors the diagnosis of VT. A negative QRS in V6 also favors the diagnosis of VT.
6) I see no AV dissociation (P waves that are not associated with the QRS complexes). If present, AV dissociation guarantees a diagnosis of VT.
While the actual differentiation between SVT and VT can be much more complicated than this, I feel that this patient has a very good chance of having SVT with LBBB that is probably rate-related. His rhythm spontaneously converted to an irregular sinus rhythm. If this tachycardia recurs or persists, an electrophysiological study could be needed to find the cause and confirm the diagnosis.
I would love to know what you think about this rhythm. In the Basic Rhythms section, I will post a strip of his multifocal atrial tachycardia.